Objectives: Indications for combined colon surgery together with other procedures include oncologic multivisceral resections and abdominal trauma and the open approach is still more commonly used. It is unclear if combining minimally invasive colon surgery with unrelated other procedures increases the risk for complications including anastomotic leakage.
Methods: The personal surgical database from two institutions during a nine year period was queried for combined colon surgeries together with other interventions. All open cases, combined cases performed for one pathology and minimally invasive colon surgeries together with a minor procedure were excluded.
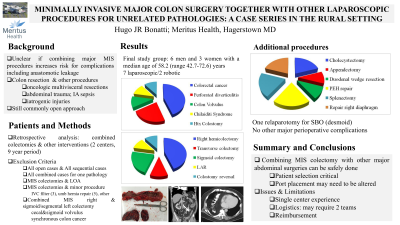
Results: The final study group consisted of 6 men and 3 women with a median age of 58.2 (range 42.7-72.6) years. There were 4 right, 2 sigmoid and one transverse colectomies, 1 rectum resection and 1 colostomy reversal; five patients had colorectal cancer, two had perforated diverticulitis and two had colonic volvulus. Additional procedures included two splenectomies (one for sarcoidosis, one for ITP), two fundoplications for a paraesophageal hernia, two cholecystectomies for chronic calculous cholecystitis, one appendectomy for acute appendicitis, one duodenal wedge resection for carcinoid and two right diaphragmatic repairs (eventration and Morgagni type hernia). Seven cases were done laparoscopic and the last two with robotic assistance. There was not a single anastomotic breakdown and no complications with regard to the second procedure.
Conclusion: Combining laparoscopic colectomy and other major abdominal surgeries can be safely done and in this limited series did not increase morbidity or mortality but safes the patient a second operation. Patient selection seems important and port placement may need to be altered to achieve good exposure for both procedures.