Objectives: Torsion of the fallopian tube is a rare diagnosis with a reported incidence of 1:1,500,000. It may be caused by an intrinsic issue (tubal lesion, hematosalpinx or hydrosalpinx) or an extrinsic issue (paratubal cyst, ovarian lesion, or adhesions). Hydrosalpinx is the most common etiology in an adolescent. Presentation is variable but commonly includes abdominal pain and emesis. Diagnosis can be difficult due to general symptoms and inconsistent findings on imaging. Delays may lead to salpingectomy.
Methods: A case series of adolescents with fallopian tube torsion treated at our institution over the last calendar year is presented. Chart review was performed retrospectively on these patients for information pertaining to preoperative symptoms, imaging, operative management and fallopian tube salvageability.
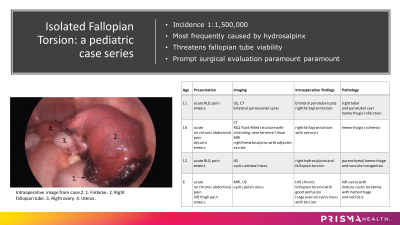
Results: Four patients with fallopian tube torsion were identified. Two patients presented with acute on chronic abdominal pain due to a known or suspected pelvic cystic mass. The other two patients both presented with acute onset of right lower quadrant pain and emesis. All four patients underwent ultrasound and cross-sectional imaging with CT or MRI. A pelvic cystic mass was identified in all four cases. Diagnosis of fallopian tube torsion was not definitively made with radiographic studies in any individual. All four underwent diagnostic laparoscopic evaluation and were found to have torsed fallopian tubes. Paratubal cysts were identified in one, a large ovarian cystic mass in another and hydro/hematosalpinx in the other two patients. In three of four cases the fallopian tube was found to be ischemic, despite detorsion, and each patient underwent salpingectomy. The patient with an ovarian lesion required oophorectomy but had preservation of fallopian tube, and ovarian pathology showed the lesion to be a mature cystic teratoma.
Conclusion: This case series serves to demonstrate the difficulty with diagnosing fallopian tube torsion in an adolescent. Like ovarian torsion, torsion of the fallopian tube is difficult to diagnose radiographically. The most common finding in our series was a cystic mass in the pelvis which can be found on ultrasound. This should prompt urgent surgical evaluation in a patient presenting with acute onset of abdominal pain. Delays for further cross-sectional imaging may not confirm a diagnosis and can contribute to loss of the fallopian tube. Our series reinforces current literature recommendations for emergent diagnostic laparoscopy with attempt at detorsion to restore blood flow to salvage the fallopian tube, and salpingectomy when the cause of torsion is thought to be irreversible or harmful to the patient.