Trauma Surgeon Atlanta Medical Center, United States
Objectives: Racial disparities in violent victimization are widely recognized, but knowledge of underlying causes (such as structural violence) is not universal. In teaching future generations of surgeons, emphasis of victim-blaming explanations of injury may undermine investment in prevention, particularly if no interventions are discussed. This study presents an analysis of trauma surgery textbooks that systematically describes types of preventative interventions and underlying causes discussed for passages that mention injury prevention or disparities.
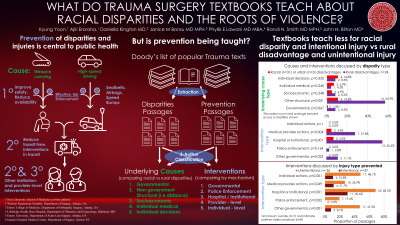
Methods: Trauma textbooks that were not technical guides or atlases were drawn from Doody’s list, an industry-standard list of resources used by medical libraries. Passages that discussed trauma injury prevention, racial/ethnic disparities or urban/rural disparities were extracted. Passages were classified by the type of injury and disparity discussed, types of intervention discussed (legislation/direct government action, law enforcement, or institution/provider level), and types of underlying causes discussed (legislation/governmental policy, socioeconomic factors, other structural factors, individual medical, or individual behavioral). Z tests were performed to compare findings by injury type (violent vs. unintentional) and affected disadvantaged group (minorities vs. rural populations). Two authors performed classifications and Cohen’s Kappa was calculated to assess agreement.
Results: 146 passages were extracted from 7 textbooks, totaling 5576 pages of text. Structural underlying causes were infrequently mentioned in the context of disparities, particularly compared to discussion of individual choices. Also, passages discussing racial disadvantages were less likely than those discussing rural disadvantages to mention the underlying role of government policy (0 vs 12%, p=0.041). Passages discussing prevention of violent injuries were less likely than those discussing accidental injury to mention governmental (12% vs 50%, p = 0.006) or institutional interventions (35% vs 72% p=0.017). Passages discussing racial disadvantages were less likely than those discussing rural disadvantages to mention institutional or clinical preventative interventions (15% vs 68% p=0.0004). Overall inter-rater agreement was 90% with a Kappa of 0.67.
Conclusion: Trauma surgery textbooks may underemphasize the role of structural factors in contributing to risk of injuries by any mechanism. Furthermore, structural and governmental interventions are more likely to be endorsed to prevent accidental injuries. Interventions to address racial disparities were infrequently described, particularly when compared to passages discussing rural disadvantages. Future textbooks should discuss evidence for preventative interventions for both racial disparities and violent injuries.