Objectives: A Patent Foramen Ovale (PFO) is present in approximately 27-35% of the population. Presence of these right to left cardiac shunts predisposes patients to cerebrovascular accidents and other arterial emboli in the presence of venous thromboembolisms. Suspicion of a paradoxical embolus should be high in patients presenting with acute pulmonary embolus (PE) or deep venous thrombosis (DVT) and arterial emboli.
Methods: A 45-year-old male with protein C deficiency and history of DVT presented to the emergency department with a week-long history of vague chest pain, shortness of breath, and acute onset of left arm numbness. CTA showed a massive saddle PE along with arterial emboli involving the aortic arch, left common carotid artery, and left subclavian artery. Systemic anticoagulation with heparin was initiated and Vascular Surgery and Interventional Cardiology were consulted for further evaluation and treatment.
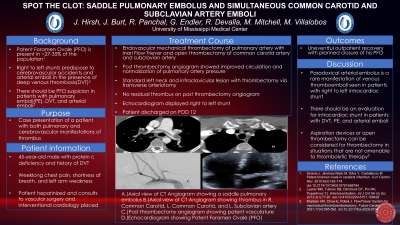
Results: After a multidisciplinary discussion, the decision was made to proceed first with an endovascular mechanical thrombectomy of the pulmonary artery for the large life-threatening PE, followed by open thrombectomy of common carotid and subclavian arteries. The endovascular mechanical thrombectomy was performed via percutaneous femoral vein access using the Inari Flow Triever thrombectomy system. After successful thrombectomy, pulmonary angiography showed significant improvement in pulmonary arterial blood flow and normalization of pulmonary artery pressures. After stabilization, the patient underwent open thrombectomy of the left carotid and subclavian arteries. Exposure of the left carotid vessels and left axillary artery was obtained through a standard left neck incision and a separate left infraclavicular incision. The thrombectomy was performed via transverse arteriotomies in the common carotid and axillary arteries. Completion aortography showed no residual thrombus in the left subclavian and common carotid arteries. The patient did well postoperatively and was discharged on POD 12 without any complications. Echocardiogram confirmed a right to left intra-cardiac shunt consistent with a PFO which will be closed after he recovers from this acute event.
Conclusion: Paradoxical arterial embolus is a rare manifestation of venous thromboemboli in patients with a right to left intra-cardiac shunt and may have devastating consequences. There should be a high degree of suspicion for paradoxical emboli in patients with arterial emboli in the setting of DVT and PE.