PLASTIC SURGERY RESPONSE TO CRANIOFACIAL TRAUMA IN A RURAL STATES TERTIARY CARE LEVEL I TRAUMA CENTER: ASSESSING THE NEED FOR TRANSFER FOR ISOLATED INJURY.
Trauma / Critical Care Surgeon Maine Medical Center / University of New England, United States
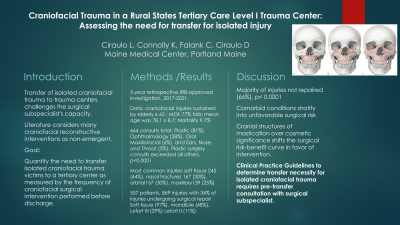
Objectives: In a rural states trauma system with one verified Level one center, the management of craniofacial injury defaults to the plastic surgeons providing care to the institution. The transfer of isolated craniofacial trauma to these centers challenges the plastic surgeons capacity to provide care for these victims while providing support for none traumatic demands for their expertise in the community. This manuscript quantifies the need for transfer of craniofacial trauma victims as measured by the frequency of surgical intervention upon these patients prior to discharge.
Methods: A retrospective 5 year review (2017-2021) of craniofacial trauma patient’s ≥65 years old admitted to a rural level I Trauma Center was conducted. Assessment of the frequency of surgical intervention by plastic surgery consultants during the patient’s hospitalization as a measure of necessity for consultation was investigated. In addition the type of intervention performed, and laceration repair verses craniofacial reconstruction were quantified. . Statistical analysis was conducted using ꭓ2 in R Studio with p≤0.05 as statistically significant.
Results: A total of 557 craniofacial injuries were identified from a population with a mean of 78 years of age. Twenty percent of patients had a plastic surgery intervention during hospitalization, p < 0.0001. Of those 20% interventions only 22% had craniofacial reconstruction with the remaining being laceration repair, p < 0.0001. Fifty-eight percent of the patients were transferred in from an outside hospital or other facility. Sixteen percent of transferred in patients had surgery with 26% of those being craniofacial reconstruction, p < 0.0001.
Conclusion: With less than 20% of all craniofacial trauma victims requiring surgical intervention acutely, a more refined screening process for in hospital consultation and indication for outside hospital transfer should be established. This limited retrospective data would suggest orbital entrapment and LeForte type injuries favor intervention prior to discharge. Developing a measured assessment of indications for transferring craniofacial trauma patients to tertiary centers could potentially help reduce the burden upon trauma systems and the time demand on the already limited availability of plastic surgeons.