Background: Tocilizumab did not improve COVID-19 survival in the COVACTA randomized clinical trial (RCT). Clinical RCT entry criteria enroll so many study drug non-responders that treatment effects are diluted. This may have affected COVACTA. The SMART methodology identifies drug-responsive patients within RCT’s
Objective: To identify COVACTA patients among whom tocilizumab reduced COVID-19 mortality
Methods: On de-identified data from 438 COVACTA patients (144 placebo, 294 tocilizumab) pre-randomization stepwise logistic regression survival models were built separately for placebo and tocilizumab within three cohorts: 1. All COVACTA patients 2. COVACTA patients receiving steroids before/during the study. 3. No steroids. Pre-randomization data from all patients were entered into both models. Model interactions with 28-day survival determined optimum cutoffs, incrementally excluding from efficacy analysis patients predicted to be tocilizumab non-responders
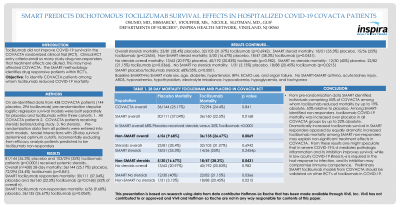
Results: 81/144 (56.3%) placebo and 103/294 (35%) tocilizumab patients (p < 0.0001) received systemic steroids.
Baseline SMART>No SMART male sex, age, diabetes, hypertension, BPH, ECMO use, and organ failure. NoSMART>SMART asthma, acute kidney injury, ARDS, hyponatremia, hypothyroidism, electrolyte imbalance, hypocalcemia, hypoglycemia, and tachypnea
Conclusion: From pre-randomization data SMART identified individuals comprising 55% of COVACTA among whom tocilizumab reduced mortality by up to 19% absolute, and 53% relative to placebo. Among SMART-identified non-responders, tocilizumab COVID-19 mortality was increased over placebo in all COVACTA groups by up to 22% absolute. Dramatically increased tocilizumab survival in SMART responders opposed by equally dramatic increased tocilizumab mortality among SMART non-responders may explain non-significant treatment effects in COVACTA. From these results, one might speculate that in severe COVID-19 IL-6 mediates pathologic inflammation and its inhibition improves survival, while in low acuity COVID-19 illness IL-6 is required in the host response to infection, and its inhibition may compromise immune competence. Preliminary SMART tocilizumab models from COVACTA should be validated on other RCT’s of tocilizumab in COVID-19